
Fluency Shaping Techniques
-
Finding Help
-
Stretched Syllables
-
Relaxed Breathing
-
Phonation
-
Reduced Articulatory Pressure
-
Knowledge of Results (Feedback)
-
The Evidence
Fluency shaping therapy teaches
- relaxed, diaphragmatic breathing
- slow speech with stretched vowels and voiced consonants
- vocal fold awareness and control
- relaxed articulation (lips, jaw, and tongue)
Fluency shaping techniques are not normal speech. Fluency shaping speech sounds “weird.” The idea is to go to extremes when practicing (in the speech clinic or at home), and then in “real world” conversations you reduce the techniques so that you sound normal and speak fluently.
Finding Help
Speech is about talking to other people. You can’t improve your speech alone. Ask for help.
Find a Fluency Shaping Program
An intensive residential program is good way to learn fluency shaping:
Each program takes about two weeks.
Find a Fluency Specialist
Finding a speech-language pathologist (SLP) who treats stuttering with Evidence-Based Practice (EBP) isn’t easy.
The American Speech-Language-Hearing Association (ASHA) ProFind webpage will find SLPs who treat fluency disorders.
The American Board of Fluency and Fluency Disorders has a search page for finding board certified Fluency Specialists.
Spero Stuttering lists SLPs who’ve pledged to be “Allies of Stuttering.” This includes pledging to practice “research-based” therapies.
Contact a local support group associated with a national stuttering self-help organization and ask for recommendations. In the United States the National Stuttering Association has local support groups. The International Stuttering Association maintains a list of self-help organizations around the world.
Some SLPs provide ineffective, non-scientific therapies that maximize their income, not your fluency. These charlatans want you to come back twice a week at $200 a session for months or years. Or they’ll tell you to take out a second mortgage to pay for a device that does nothing for you, but makes them thousands of dollars in profits. They justify their scams by saying that they do the same therapies that other SLPs are doing. Charlatans do what other charlatans do.
Find a Support Group
I may be old-fashioned but I prefer in-person support groups to online support groups. The Facebook support groups I’ve seen are dominated by people who make negative insubstantial comments (“trolls”). When someone asks if a therapy works, the trolls jump in and say “That doesn’t work.” When a new member asks for advice for what therapy to do the trolls jump in and say “Nothing works!” The trolls drive away everyone else.
The National Stuttering Association has in-person support groups for adults and teenagers. Their annual convention, usually in July, is well-attended.
Is Self-Therapy an Option?
You can learn cognitive stage motor skills from a book or video. Analogously, many videotapes offer to teach golfers how to improve their swing.
The associative stage requires feedback. A trained individual must observe you and tell you when your performance is correct, when your performance is incorrect, and what to change to correct your performance.
Stretched Syllables
Slow speech is not a fluency shaping target. This is slow speech:
“I” < pause> “am” < pause> “an” < pause> “American.”
Saying “I am an American” normally takes about 1.5 seconds (seven syllables at about five syllables per second). By silently pausing two seconds between words, and saying each word normally, the phrase would take about eight seconds. That wouldn’t improve your fluency.
Instead, stretch each syllable a second or two. Stretch vowels and voiced consonants (e.g., /m/, /n/, /r/). Articulate voiceless consonants (e.g., /k/) lightly and quickly, just touching your lips or tongue and then moving to the next voiced sound.
Join the syllables together, with no breaks or pauses between words. The result should sound like:
“IIIIIIIIaaaaammmmaaaaannAAAAAmmmmeeeeerriiiiiiiikaaaaann”
Stretch each syllable equally. In other words, “American” should take four times longer to say than “I.” Don’t make “American” the same length as “I.”
Start with stretching each syllable two seconds. When you’re 100% fluent at two-second stretch you can go to one-second stretch. If you stutter even once on one-second stretch, go back to two-second stretch.
A speech-language pathologist measured my fastest speech (reading aloud alone) at ten times slower than persons who don’t stutter. He then taught me fluency shaping. I talked fluently five times slower than persons who don’t stutter. My speech was slow compared to persons who don’t stutter but was faster than stuttering. Slow speech is not a fluency shaping target.
Relaxed Breathing
Place one hand on your stomach. Breathe so that your hand moves out when you inhale, and in when you exhale.
Notice that you’re taking many small breaths. Your inhale and exhale times are equal.
This is relaxed or diaphragmatic breathing. This is the way people normally breathe.
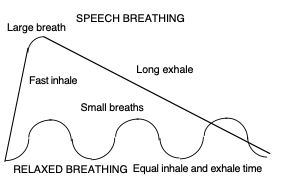
Upper chest or thoracic breathing increases our lung capacity. It enables us to maximize our physical exertion. Our “fight or flight” instinct switches us to thoracic breathing. Thoracic breathing starts with a big breath, using your upper chest muscles to expand your lungs. Release the air slowly, while maintaining this upper chest muscle tension to hold air in your lungs as long as possible. When you’ve released the air, quickly take another breath, filling your lungs as rapidly as possible.
Some individuals hyperventilate or switch to thoracic breathing when experiencing non-physical stress. Stress reduction classes teach students to relax by switching to diaphragmatic breathing.
We use thoracic breathing when talking. A large breath with a long, slow exhale enable us to speak many words before pausing for another breath.
Well-meaning people who know nothing about stuttering may tell you to “take a deep breath” before talking. But the opposite is better advice. Diaphragmatic breathing is practiced in fluency shaping and other stuttering therapy programs. Taking smaller breaths with your diaphragm can help you relax and talk fluently.
Try it. Diaphragmatic breathing will relax your vocal folds, and then your lips, jaw, and tongue. Your voice will deepen and sound confident and even “sexy.” You’ll feel relaxed and confident.
Practice a word list or read a magazine page aloud using diaphragmatic breathing.
You’ll soon discover a few problems trying to speak with diaphragmatic breathing. Each breath is small, so you’re able to say only a few words on each breath. Inhale time and exhale time are equal, so you have long pauses between short phrases. You’re unable to speak loudly.
Like other fluent speech motor skills, speaking with diaphragmatic breathing is abnormal but useful. Include speaking with diaphragmatic breathing in your stuttering therapy practice exercises. Mastering this skill will enable you to speak short phrases fluently in stressful situations. For example, a police officer pulls you over for speeding. You don’t need to say much besides, “Yes, officer,” and “No, officer.”
Phonation
Your vocal folds are flaps of muscle in your throat. Making your vocal folds vibrate produces sound. This sound then becomes your voice. Vocal fold vibration is called phonation.
Two conditions produce phonation. First, you release air from your lungs. Next, you tension or tighten your vocal folds.
Place your fingers on your throat. Exhale and hum. Your fingers should feel a vibration. This is your vocal folds vibrating.
Stop humming, and feel the vibration stop. Practice switching your phonation on and off.
Now vary your phonation in two ways:
- Change your volume (hum louder, then quieter).
- Change your pitch. Hum up and down a musical scale.
How did you do that? You varied your volume of exhalation, i.e., you increased or decreased the air releasing from your lungs by tensing or relaxing your thoracic (upper chest) muscles. More exhalation enabled you to produce more volume.
You also varied your vocal fold tension. Tense vocal folds produce a higher-pitched voice. Relaxed vocal folds produce a deeper or lower-pitched voice.
Tense your vocal folds as hard as you can. You’ll block your throat, not allowing any air to escape. If you take a deep breath and then block your throat, your increased lung pressure makes your chest stronger. Like inflating a tire to carry a heavier load, this is effective for lifting a heavy weight. But it’s not a good way to talk!
Practice one more aspect of phonation. Take a breath and hold it, tense your vocal folds, then release air. Switch to the other way: take a breath, release a little air, then tense your vocal folds. Note that the former produced a croak. The latter produced a nice hum. This shows that phonation requires timing two muscle movements: exhaling a little air, and then starting to tense your vocal folds.
You see that three things can go wrong with phonation:
- Releasing too much or too little air (inadequate breath support).
- Overtensing your vocal folds. Under stress, you may try too hard to talk, tense your vocal folds too much, and block off air flow. This results in a silent block.
- Mistiming exhalation and vocal fold tension. A goal of stuttering therapy is train the stutterer to consciously breathe, release a little air, gently tense his vocal folds, and then begin to talk. This exercise is called gentle onset or easy onset.
Gentle Onsets with Vowels
To hit a baseball home run, you use all of your arm muscle strength. In contrast, to putt a golf ball a few feet, your arm muscles are more relaxed than tense. Phonation is like putting a golf ball, not hitting a home run.
To use gentle onsets (also called easy onsets), take a relaxed breath with your diaphragm. Release a little air and say ah as you gradually increase vocal fold tension. Feel your vocal folds begin to vibrate. Increase your vocal fold tension, until you reach normal speaking volume. Gradually reduce vocal fold tension, until you’re silent. Time this to take about two seconds. You should be able to do this on one breath, without reaching residual air.
You can buy computer applications that graph your phonation contour. Applications include Dr. Fluency, Speak:Gentle, and the Computer-Aided Fluency Establishment and Trainer (CAFET). Or you can use a sound-recording and -editing application (many such applications are available free). On a computer monitor, your vocal volume should look like this:
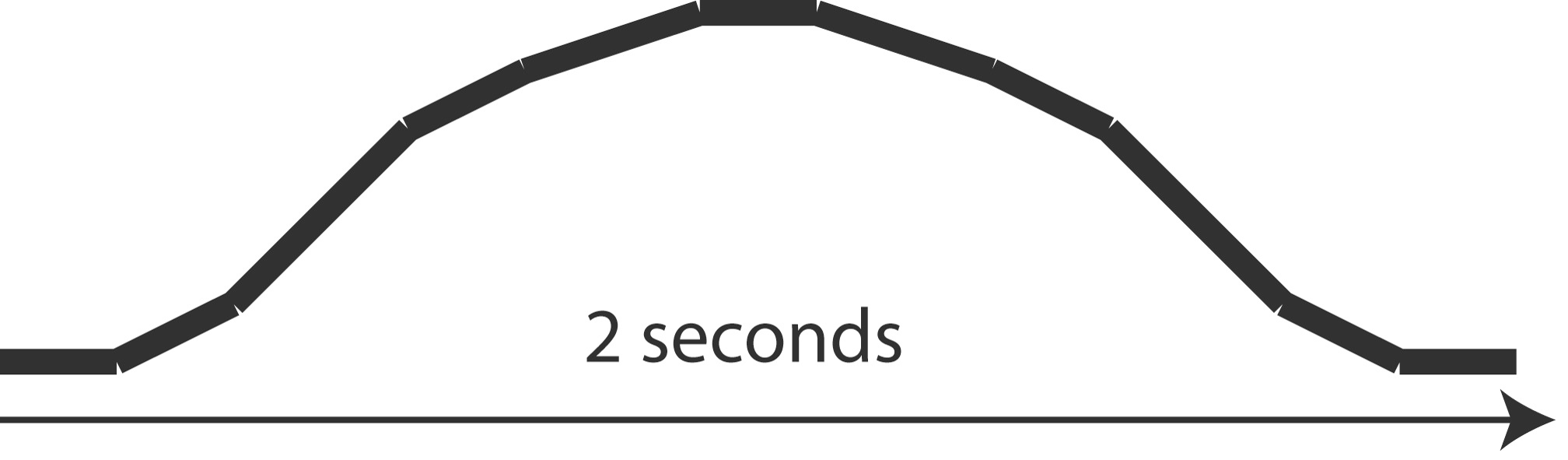
Gentle onset voice contour
Practice fifteen gentle onsets with the fifteen vowel sounds (say the vowel, not the word):
| Vowels |
| i (green tea) |
| ɪ (silver pin) |
| ə (the plum) |
| ʊ (wooden hook) |
| u (blue moon) |
| æ (black cat) |
| ɛ (red bet) |
| ɛɹ (square) |
| ɚ (purple shirt) |
| ɔ (auburn dog) |
| ɔɹ (door) |
| ɑ (blonde) |
| ɑɹ (dark star) |
| Diphthongs (two vowels produced together) |
| eɪ (gray jay) |
| oʊ (rose boat) |
| ɔɪ (turquoise toy) |
| aɪ (white tie) |
| aʊ (brown cow) |
I’ll bet you didn’t know that American English has 18 vowels!
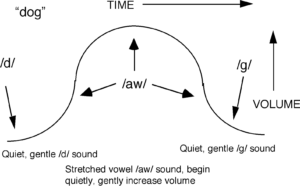
Gentle Onsets with Words
Now say “dog,” stretched over two seconds, with gentle onset. Begin with a quiet, gentle /d/ sound. Switch to the /aw/ vowel sound and gradually increase vocal volume. After one second, gradually reduce vocal volume. Switch to the /g/ sound, and stop vocal fold vibration.
Voiced and Voiceless Consonants
All vowels are voiced. To produce vowels you vibrate your vocal folds (phonation) and then move your lips, jaw, and tongue to make the vowel.
Many consonants come in voiced/voiceless pairs. Voiced consonants are produced by vibrating your vocal folds while moving your lips, jaw, and tongue. Voiceless phonemes are produced with the same lips, jaw and tongue movements but without vocal fold vibration.
Put your fingers on your throat and make the consonants. You’ll feel your vocal folds vibrate for the voiced consonants and not vibrate for the voiceless consonants. Stretch each word to two seconds.
| Voiceless | Voiced |
| p (pen, pad) | b (Ben, bad) |
| t (tea, cat) | d (did, cad) |
| tʃ (church) | dʒ (jam, badger) |
| k (cat) | g (get) |
| f (fall, staff) | v (voice, of) |
| θ (thin, math) | ð (father, thy) |
| s (so, less) | z (zoo, has) |
| ʃ (she, cash) | ʒ (vision, pleasure) |
| h (how, hat) | x (loch, hanukkah) |
| w (woman) | |
| l (leg, sly, gal) | |
| ɹ (rye, trap) | |
| j (yes, yard) | |
| m (man, stem) | |
| n (no, can) | |
| ɲ (canyon) | |
| ŋ (sing) |
In fluent speech your vocal fold vibration (phonation) switches on and off many times per second. For example, if you say “bad pig” you phonate on every sound except the p. In other words, your vocal folds switch on for bad, switch off for p, then switch on again for ig. The timing can be as precise as one one-hundredth (1/100) of a second.
The inability to switch your phonation on and off is a core stuttering behavior. Or, specifically, on. If you try to say “bad pig” and get stuck on the p, you’re not stuttering on the p. You’re doing a great job pronouncing the p. You’re stuttering on the i. Your problem is moving from the p to the i.
Fluency shaping solves this problem by slowing down speech to use closed-loop motor control instead of open-loop motor control to initiate phonation.
Gentle Onsets with Multisyllabic Words
Practice using a gentle onset on each syllable. Go loud on each vowel. On the consonants, relax, go quiet, and lightly and quickly articulate the sounds.
For example, on “American,” you start with a gentle onset on the initial /uh/. Open your mouth wide at the loudest point in the phonation contour.
Take the /uh/ sound down in volume, while at the same time closing your mouth to articulate the voiced /m/. Bring the /eh/ sound up in volume. Again, open your mouth wide at the loudest point in the phonation contour.
Take the /eh/ sound down in volume, while at the same time reduce your jaw opening (but don’t close your lips) to articulate the voiced /r/.
Open your mouth wide again for the /ih/ vowel on the third syllable.
Now you get to the only voiceless sound in “American.” Before the /k/ sound, take the down the volume of the /ih/ vowel. Whisper the /k/. If you block, you dropped the /ih/ volume too fast. Try again with a long, slow decline in volume on the /ih/. Articulate the /k/ lightly, for just a moment.
If you still block on the /k/, change it to a voiced /g/. In other words, say “Amerigan.”
Use another gentle onset on the final /eh/ vowel. Reduce your volume on the final voiced /n/ consonant.
The result is an abnormal-sounding “sing-song” speech pattern. Your jaw opens and closes noticeably on each syllable. While you won’t want to talk like this for the rest of your life, for practice or in stressful situations this technique helps you use gentle onsets, continuous phonation, and a slower speaking rate.
Reduced Articulatory Pressure
The third set of speech muscles (after respiration and phonation) are your articulators: lips, jaw, and tongue. These muscles form your vocal fold humming into sounds and words. If you phonate without moving your lips, jaw, and tongue, all that comes out of your mouth is humming. The goal of this last target is to relax these muscles.
Reduced articulatory pressure is also called “soft targets.”
Lightly touch your tongue for the /t/. Lightly close your lips for the /b/. Keep your speech production muscles relaxed for all sounds.
The wrong way is to tense your lips and tongue and jaw too much, and hold this tension too long.
You’ve learned to stretch and emphasize vowels. Now work on de-emphasizing consonants. If you stretch and emphasize vowels, and de-emphasize consonants, you should be able to speak fluently.
Read a word list or magazine page aloud. Feel how your lips, jaw, and tongue move to change sounds. Say each word with normal articulation tension. Then say the word again with tense articulation. Then say the word again with relaxed articulation.
Some stuttering therapy programs at this point devote many hours to teaching the stutterer the correct lips, jaw, and tongue position for each of the 40+ sounds of English. This is unnecessary, in my opinion. Stuttering is not an articulation disorder. Stutterers don’t, in general, misarticulate sounds (e.g., saying /w/ instead of /v/). Stutterers instead only need to relax their lips, jaws, and tongues. This is the easiest part of fluency shaping therapy.
Knowledge of Results (Feedback)
The associative stage of motor learning requires feedback. In sports this is called knowledge of results. For example, in golf or tennis you see where the ball goes after you hit it. Playing golf or tennis on a dark, foggy night would be difficult.
Feedback quality is affected by speed. If you hit ten golf balls on a dark, foggy night, then the next day find one of the balls 150 yards away, you’ll have no memory of what you did right to hit it so far.
Feedback quality is also affected by accuracy. If you and your buddy each hit a golf ball, and one ball goes 150 yards but you don’t know whose ball it was, you have inaccurate feedback.
Or the observer gets bored. If you hit golf balls for hours, and have a person telling you how far the balls go, sooner or later the person will stop paying attention.
Which Fluency Skills Need Feedback?
When you’re learning fluent speech motor skills, you need knowledge of results. Some skills are easy to observe. For example, resting your hand on your stomach tells you whether you’re using diaphragmatic (relaxed) breathing or thoracic (speech) breathing.
Your articulators (lips, jaw, and tongue) are a little harder to be aware of, as you can’t see them. But you have good proprioceptive awareness of these muscles, so developing awareness and control isn’t hard.
Your vocal folds are another story. These muscles are deep in your throat. You can’t touch them or see them. Most people don’t even know they have vocal folds.
The most difficult feedback is with the timing of all this. For example, your speech-language pathologist tells you to exhale a little air and then increase your vocal fold tension. You do this slowly and correctly. Then she tells you to increase the speed. You must execute these movements within hundredths of a second. You can’t tell whether you’re doing it right, and most speech-language pathologists can’t either. A fluency specialist who’s helped hundreds of stutterers has better-trained ear and visual skills and gives better quality of feedback than a speech-language pathologist who’s never treated a stutterer.
Van Riper’s Prediction
In 1974, Charles Van Riper (a stutterer and a “founding father of the field of speech-language pathology”) predicted what a future historian would say about the next hundred years of stuttering treatments:[ref]Van Riper, C. “Stuttering: Where and Whither?” Asha, vol. 16, no. 9, September 1974, page 486.[/ref]
Our scrutiny of two old books on the nature and treatment of stuttering* that were published in the early 1970s reveals a vast collection of misinformation, ignorance, and benightedness. Preventative and remedial practices were characterized by a primitiveness and crudity that now seem appalling. The lot of the stutterer at that time must have been a very sad one. Nevertheless, in the last two decades of the twentieth century, we do find some progress in solving the problems of this ancient affliction.
*Van Riper’s two books were The Nature of Stuttering (1971) and The Treatment of Stuttering (1973).
Van Riper then predicted the organization of stuttering self-help groups, a scientific journal devoted to research about stuttering, and the certification of speech-language pathologists specializing in stuttering. All of these have happened. He then predicted that a stutterer would invent[ref]Van Riper, C. “Stuttering: Where and Whither?” Asha, vol. 16, no. 9, September 1974, page 487.[/ref]
a biofeedback computer system that provided a backflow of error information from sensors that monitored [breathing, speech motor tension, and articulation errors and then] stimulated the pain centers when error signals appeared or alternatively stimulated the pleasure centers when the stutterer did not make these errors but instead spoke fluently.
[The biofeedback computer system] was able to make…adult stutterers completely fluent after just a few hours [in the speech clinic, and use of a portable device produced carryover fluency and the subjects were able to stop using the device] after only a month of intensive therapy. Despite his success, we note [that the inventor] found it very difficult to convince the stuttering specialists of his time that his invention was truly effective.
Biofeedback Devices
Biofeedback is the measurement and display to the user of a physiological activity, to enable the user to improve awareness and control of the activity. Biofeedback machines:
- Provide faster, more precise, and more reliable feedback than a human observer.
- Provide real-time feedback, beeping the instant you make a mistake.
- Provide accuracy measuring things humans can’t see or hear.
- Never get bored, even after hours of practice.
You still need a speech-language pathologist to train you to do the target motor skills (cognitive stage). The machines can only help you to refine your skills (associative stage).
I’ve spent thirty years trying to build Van Riper’s biofeedback computer system. The central problem is that your vocal folds are deep in your neck. Surface sensors on your skin can’t monitor vocal fold activity. Monitoring vocal fold activity requires using needle electrodes into your neck. Monitoring vocal fold activity with a throat microphone is workable (see Duration of Phonated Intervals therapy).
Van Riper was right that SLPs refuse to use such devices and that stutterers won’t wear such a device outside of a speech clinic.
The Evidence
A rigorous study followed 42 stutterers through the three-week program at the Institute for Stuttering Therapy and Treatment (ISTAR) in Edmonton, Alberta, Canada.[ref]Boberg, E., & Kully, D. (1994). “Long-term results of an intensive treatment program for adults and adolescents who stutter.” Journal of Speech and Hearing Research, 37, 1050-1059.[/ref] The fluency shaping program was based on slow, prolonged speech, starting with 1.5-seconds-per-syllable stretch, and ending with slow-normal speech. The program also works on reducing fears and avoidances, discussing stuttering openly, and changing social habits to increase speaking. The program includes a maintenance program for practicing at home. The program reduced stuttering from about 15-20% stuttered syllables to 1-2% stuttered syllables. Twelve to 24 months after therapy, about 70% of the stutterers had satisfactory fluency. About 5% were marginally successful. About 25% had unsatisfactory fluency.
A more recent study of the ISTAR program found that improved results, with 71-86% of graduates retaining fluency two years post-treatment.[ref]Langevin, M., Huinck, W.J., Kully, D., Peters, H.F.M., Lomheim, H., and Tellers, M. “A cross-cultural, long-term outcome evaluation of the ISTAR Comprehensive Stuttering Program across Dutch and Canadian adults who stutter,” Journal of Fluency Disorders, Volume 31, Issue 4, 2006, Pages 229-256.[/ref]
A study of Precision Fluency Shaping found that a three-week intensive program followed by one year of follow-ups reduced stuttering from 7.1% to 1.6%. A year later the average stuttering was 3.6% (a 50% reduction in stuttering).[ref]Bloodstein, O., & Bernstein Ratner, N. (2007). A Handbook on Stuttering, Sixth Edition. Clifton Park, NY: Thomson. ISBN 978-1-4180-4203-5, page 398.[/ref]
After completion of another “smooth speech” fluency shaping stuttering therapy program, about 95% of subjects were “very satisfied” or “satisfied” with their speech at the end of the treatment. A year later, their satisfaction dropped to 43%.[ref]Craig, A., Calver, P. “Following Up on Treated Stutterers: Studies of Perceptions of Fluency and Job Status.” Journal of Speech and Hearing Research, 34, 279-284, April 1991.[/ref]
Another study reported that 100% of subjects who completed a year-long “prolonged speech” fluency shaping stuttering therapy program were able to speak nearly fluently. But two-thirds of the stutterers who started the program didn’t complete it.[ref]Onslow, M., et al., “Speech Outcomes of a Prolonged-Speech Treatment for Stuttering,” Journal of Speech and Hearing Research, 39, 734-749, 1996.[/ref]
Submit your review | |